It’s time to replace employer sponsored health insurance (ESI) in the United States with a Federally funded payment system that is more efficient, more fair, and more stable.
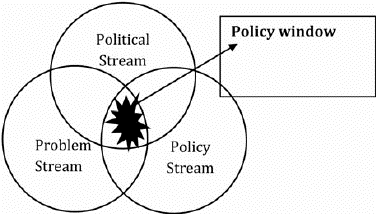
The Covid-19 pandemic driven instability in the US economy and illumination of the inadequacies of our health care system provide a unique policy window (see above figure and below discussion) for major changes in how we deliver health care and pay for it. Numerous sources have shown that health care in the United States is both more expensive and less effective in improving the health of the population than the health care systems in most if not all other high-income countries. Although there are many dimensions along which health care policy should be changed, this blog posting highlights the need to replace our employer-based health insurance program, which covers roughly half the population of the US, with a health plan structure that is more efficient, more equitable, and more stable than what we presently have.
What?
What about the employer sponsored insurance (ESI) is inefficient, inequitable, and unstable? In a 2019“Viewpoint” in JAMA, Victor Fuchs provides some relevant observations and their implications:
- ESI enrollment is positively correlated with income as 84% of households with income levels greater than 400% of the Federal poverty level receive employer-based health insurance. For those whose family income is less than 250% of the Federal poverty line, only 35% have ESI.
- Higher income enrollees receive the vast majority health insurance exemptions from income taxes. The exemption generates $300 billion annually in reduced taxes. “In dollar terms, the lowest-income households will get an average benefit of about $160 this year, while the highest-income taxpayers will receive an average of $4,700.”
- As a result
- the US health care system is skewed to meet the preferences of high-income employees and their families who tend to favor a fee-for-service based emphasis on specialty care with expensive technology rather than primary care and
- health care research funding has gone toward extending this expensive product mix rather than toward one focused on lower cost, disruptive innovations in care delivery based on both primary care and public health to better serve the population at large.
- Though not cited by Fuchs, the above forces tend to lead to concentrated private insurance and hospital dominated care systems in many local markets. (See Martin Gaynor’s publications, such as in JAMA, and testimony for details. )
So What?
Under stable economic conditions, the US hospital dominated care systems leave many uninsured and others under-insured, and despite having insurance, many can’t afford to seek care. Prior to March 2020, the number of uninsured in recent years had stabilized at roughly 30 million people, which certainly is more efficient and equitable than 50 million or so who lacked insurance prior to passage of the 2010 Affordable Care Act. When the economy goes into recession, however, especially in response to a pervasive pandemic, the inefficiencies and inequities of the US health care system come into full view.
- Many more people become unemployed and often uninsured.
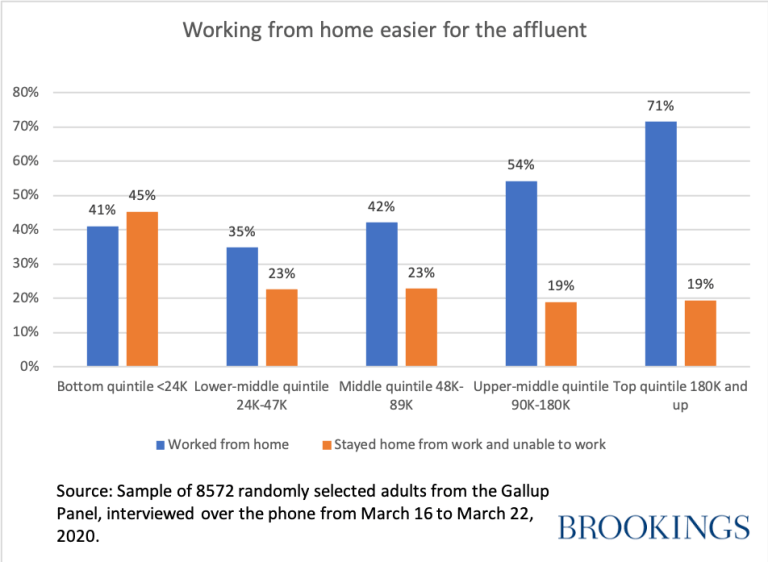
- Those with low income jobs typically can’t work from home. Unless their jobs are labeled essential, workers are likely to become unemployed because their places of employment have been closed by state decree; thus, most no longer have health insurance. Dingle and Neiman have estimated that only 37% of jobs in the U.S. can be done at home and that 46% of the wages earned come from such jobs. The disproportionate impact on adults in the lower forty percent of income groups becomes clear from the recent Gallup poll displayed below.
- During such economic downturns, for those who become unemployed, persistent efforts are needed to obtain, with a possible lag of numerous weeks, health insurance or unemployment compensation. During the present pandemic, such efforts become especially burdensome, given the lack of governmental workers to help secure these benefits.
And So?
- In the midst of the Covid-19 pandemic, more and more people are struggling to afford care for themselves and their families and to obtain needed medical care.
- Many low-income employees labeled “essential” face higher risk of infection than those who can safely hibernate at home while doing their jobs.
- The foregone tax revenue that benefits relatively well-off households could be used to create truly universal coverage funded by a less exemption filled Federal income tax.
Political scientist John Kingdon highlights the window of opportunity for policy entrepreneurs to propose and advocate for significant change in how public policy is designed and implemented. As displayed above, he argues that three ‘streams’ must be aligned for a matter to be dealt with in the public policy arena:
- the problem stream (is the condition considered a public policy problem?),
- the policy stream (are there policy alternatives that can be implemented?), and
- the political stream (are politicians willing and able to make a policy change?).
- When these three streams come together, a window of opportunity opens, and creative policy entrepreneurs can shape public policy to address the problem at hand.
All three streams are relevant at present:
- As argued above, an employer-based insurance system is both inefficient and inequitable in times of economic and health insecurity; thus, clearly a public policy problem exists.
- There is no shortage of policy alternatives. Along with other publications, Health Affairs, JAMA, and the New England Journal of Medicine have devoted numerous issues of their journal to such alternatives over the past forty years.
- The relevant question is: do we have the political will to resist the influence of powerful stakeholders for our inefficient, inequitable, and unstable health care financing and delivery system and to design and implement a stable, efficient, and fair health care system?
Employer sponsored insurance came into being as a for employers to bypass the wage and price control restrictions imposed during World War II, and it became embedded in our tax system with the Internal Revenue Act of 1954. This policy has outlived its usefulness. The time for change is now.
If Not Now, When?

This is really good.
William McLaughlin wjmcl@me.com
>
LikeLike
Thanks, Bill
LikeLike
Bring down the cost and the poor will purchase it. That’s the only solution, if it exists. Taking one of the most expensive things in the world that grows more and more expensive at a rate exceeding the exorbitant rate of higher education and making it universal is monumentally suicidal to civilization.
Or put another way, demand exceeds supply, much like residential property ergo homelessness. Let’s make residences universal while we’re at. Anybody that wants to live in Washington D.C. gets to live in Washington D.C. Same thing with Miami Beach or Aspen or any other place people want to live. It’s impossible so mandate it. Brilliant.
LikeLike